
Originally featured in Healthcare Design Magazine, February 2020.
A new cancer center opens only to require renovations six months later because volumes weren’t understood prior to construction. A health system kicks off a hybrid operating room addition without first identifying what services would be performed in that space. A multicampus health system moves forward on consolidating services in a new facility only to learn that an older building is better suited to its programmatic needs. These examples of failed master planning were encountered in just the last six months, and they’re not unique.
As the healthcare industry faces massive business changes, the master planner’s approach must also adapt. Shifting reimbursement policies and higher costs are shrinking margins, while a scaling marketplace is threatening the survival of independent hospitals. On top of this dynamic economic backdrop are educated patients whose demand for accessibility, affordability, and reputability is driving “retailization” within healthcare. Greater numbers of procedures are being performed in outpatient settings as interventional and diagnostic procedures are uncoupling from hospitals, such as office-based cardiac catheterization labs. Consumers also have access to a host of preemptive and convenience-driven options for identifying health problems, such as the use of smart devices to diagnose an ear infection, take an EKG, or detect breast cancer, which alleviate some of the need for costly diagnostic testing and even healthcare intervention.
All these factors present significant challenges for healthcare facility planners determining what to build, if to build, and where to build. That’s why delivering the maximum value possible through master planning is more important than ever.
Four primary perspectives drive how health systems make decisions and evaluate options: strategy, finance, operations, and facilities. Master planners should be focusing their work on available measurements across these perspectives, such as population growth, operating income projections, existing facility condition ratings, and operational assessment scores. However, this is where traditional master planning falls short, because it frequently doesn’t consider how these factors are integrated. Rather, the traditional master planning approach aligns strategy and finance as a precursor to determining the specifications for a facilities roadmap, later executing on the strategy with capital expenditure. Analyzing these two perspectives before addressing facilities and operations is a mistake. Facilities necessarily tie back into finance as budgets and project realities interface—and this is where architects risk failing their clients.
![Lack of Integration[1]](https://blog.array-architects.com/hs-fs/hubfs/Lack%20of%20Integration%5B1%5D.png?width=2667&name=Lack%20of%20Integration%5B1%5D.png)
Strategy is particularly problematic, as it’s rarely revisited once established. The result is that buildings—constructed long after strategic decisions inspired their programs—may open in entirely new realities. Conditions such as shifting reimbursements, encroaching competitors, or mergers and acquisitions could each have a direct impact on the longevity or usefulness of a new program. Architects (as a result of carrying out the wishes of health systems) have been responsible for buildings with purposes that have shifted and no longer align with market realities, requiring changes soon after their opening. In this traditional master planning paradigm, operations and the need to adapt to new systems of care are essentially left out of the equation.
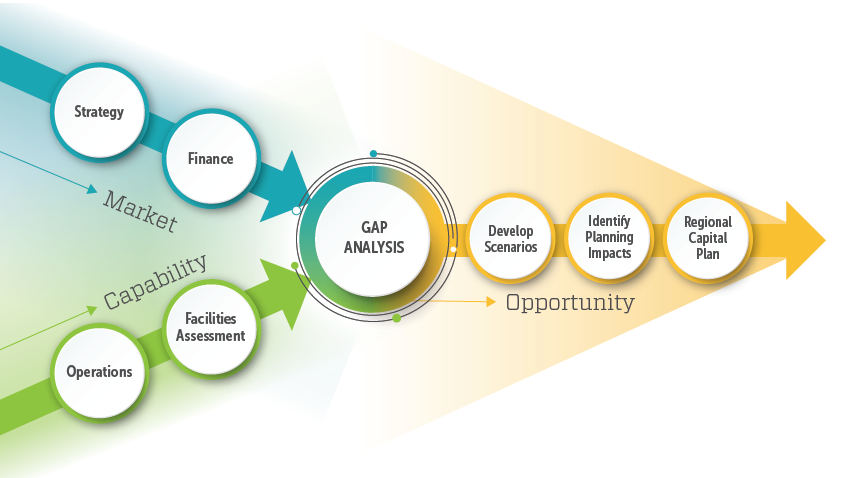
![Four perspectives[1]-1](https://blog.array-architects.com/hs-fs/hubfs/Four%20perspectives%5B1%5D-1.png?width=261&name=Four%20perspectives%5B1%5D-1.png) What if master planners led an approach that brought the conversations and experts driving the inputs of finance, operations, strategy, and facilities together? Architects are trained to challenge conventional thinking and tasked every day with leading the coordination of multiple groups with siloed expertise to align and integrate those skill sets in a way that derives a comprehensive end product. If they could help drive these conversations to happen in parallel during master planning, so all factors are considered as they push and pull one another, could it derive a more holistic solution?
What if master planners led an approach that brought the conversations and experts driving the inputs of finance, operations, strategy, and facilities together? Architects are trained to challenge conventional thinking and tasked every day with leading the coordination of multiple groups with siloed expertise to align and integrate those skill sets in a way that derives a comprehensive end product. If they could help drive these conversations to happen in parallel during master planning, so all factors are considered as they push and pull one another, could it derive a more holistic solution?
Put to the test
The team at Array Architects has been testing the hypothesis that early integration would drive more value and applying it in practice to several master planning engagements. Here are some notable findings:
- All current-state baselines can be established at the same time. Existing conditions, including budgets, marketplace, real estate, care models, etc., represent a context, or baseline, for decision-making and projecting viable strategies. Master planning shouldn’t just be about receiving strategy and financial goals, and then providing phased capital expenditures for facilities as a means of conveying that strategy. By exploring current-state baselines at the same time (including those in strategy, finance, operations, and facilities) instead of determining two as precursor to the rest (as is typical), master planners can perform much more sophisticated analyses and determine how operational and facility-based considerations alter strategy.
- An integrated approach doesn’t necessitate working within a single organization. It’s necessary to have a “conductor” (possibly the architect/master planner) driving collaboration between all parties. This conductor should be well-suited to coordinate external consultants, including strategy advisers, financial consultants, the facilities team, and operations specialists, to orchestrate a collaborative master planning engagement. Unlike the traditional approach, where health systems assume they should work out the primary strategy drivers or perform a financial analysis before engaging the master planning team, an integrated approach is a coordinated, concurrent exploration of all drivers in the equation. It’s not necessary to have all perspectives evaluated under one roof, but an ongoing conversation among all parties must occur so that decisions and information cycle through, providing influence and comparison across the perspectives. For example, macro approaches to operations have a direct impact on capacity, throughput, and need, which would influence decisions around facilities.
- An integrated approach takes the same amount of time as a traditional one. Working out primary strategy and financial drivers concurrently with operations and facilities helps health systems integrate those considerations early on to produce more rapid analyses and, in turn, a more holistic and fruitful master plan. Fortunately, an integrated approach takes the same amount of time, too, yielding a result that’s better informed and tested.
Case study
Array was engaged by a health system in the Northeast to quantify the obsolescence of an existing hospital campus and help define the system’s future through a revised inpatient and ambulatory strategy and site selection assessment. Through a multiperspective approach, the team uncovered critical information, including a sociodemographic shift occurring within the client’s market and unsustainable operational costs at key facilities, that showed the health system needed a holistic and system-wide solution. Array then integrated strategic advisers, architects, and data analysts to simultaneously evaluate program scenarios, the system’s current state, real estate assets, demographics, and strategic goals.
By evaluating these components in unison, the team was able to forgo a solution that addressed only one problem in favor of tackling foundational issues at a macro level, identifying the need for a redistribution of care resources and a new facility in an alternate location. Moreover, the team was able to determine this need using a process that demonstrated how it would lead to a higher return on investment. Lastly, our team helped the client develop alternate options to redeploy, repurpose, or reinvent its existing hospital using third-party investor, hospital, and township resources—options now being considered as a way to help the existing facility continue to serve an important community function.
Once the decision was made to move forward with a new facility, the team defined care models that complemented strategic goals; analyzed transformational options for a greenfield hospital site; planned sequential renovations of existing facilities; and defined a roadmap for operational, financial, and project success. Performing this work as an integrated team helped the client identify necessary business changes, including the transition to different sites and catchment areas. It also allowed the system to identify the lowest cost/highest impact care elements, understand which services to offer by determining volume, and serve the population in a manner that’s reflective of need.
Alternately, if this work had been performed using a conventional planning method, a hospital could have been built to a program that didn’t reflect the need in that location or allow for future flexibility, and the existing hospital campus could have been abandoned without the necessary study to determine how best it could support the community in the future.
There's no crystal ball
The four critical perspectives of strategy, finance, operations, and facilities necessary for holistic evaluation of a strategic direction in healthcare benefit from an iterative testing approach. The value of integrating master plans is that it ensures the right answers are discovered, and the right decisions are made along the way because one impacts and influences the other. Healthcare architects are uniquely suited to drive this value equation for health systems.
To make this integrated practice a reality, it will be necessary to challenge an existing paradigm. Today, when changes happen to projects, or when less-than-comprehensive studies occur and additional problems result, architects are paid to address those changes. To better serve our clients, perhaps we must admit this paradigm has sometimes hindered our clients but benefitted us—in fact, at this juncture in the healthcare industry’s evolution, it’s imperative.
As the industry rocks between mass consolidation and splintered, individualized care, healthcare architects will either be helping to navigate the ship or left in the wake. If architects are helping to drive more informed, holistic solutions for healthcare systems, in many cases, they will be decreasing construction and increasing efficiency and return on investment. Therefore, the architect’s value to those institutions increases, and the projects constructed better fulfill the needs of the community, saving money, time, and other precious resources.